
Cancer and neoplasms
Awareness of head and neck cancer among patients attended at a regional referral hospital in Tanzania
Aug
Socio-demographic characteristics of the respondents
In this study, a total of 315 respondents were recruited where majority were from rural area, 175(55.6%) while those from urban area were 140(44.4%) respondents. Males, 209 (66.3%) predominated in this study and females were 106 (33.7%) (M: F = 1.94:1). Majority of the respondents belonged to the age group, 18– 33 years (52.7%) and the least number were aged ≥ 50 years, 50(15.9%). Regarding marital status, majority of the respondents were married, 256(81.3%) while 6(1.9%) were widowed. In terms of level of education, most respondents had primary level education, 169(53.7%) and 14(4.4%) had college education. (Table 1).
History of exposure to risk factors for head and neck cancer among respondents (N = 315)
Majority of the respondents, 295(93.7%) were non-smokers and the least number of study participants were former smokers, 15(4.7%). Regarding history of orogenital sexual practice, most respondents had no prior history of orogenital sexual practice 314(99.7%). Similarly, 245(77.8%) respondents had no history of alcohol consumption and all the respondents had no prior history of chewing/sniffing tobacco (Table 2).
Awareness on head and neck cancer among the study participants
In this study, 173(54.9%) respondents considered themselves to be somewhat knowledgeable on head and neck cancer while 9(2.9%) considered themselves to be extremely knowledgeable on head and neck cancer (Table 3).
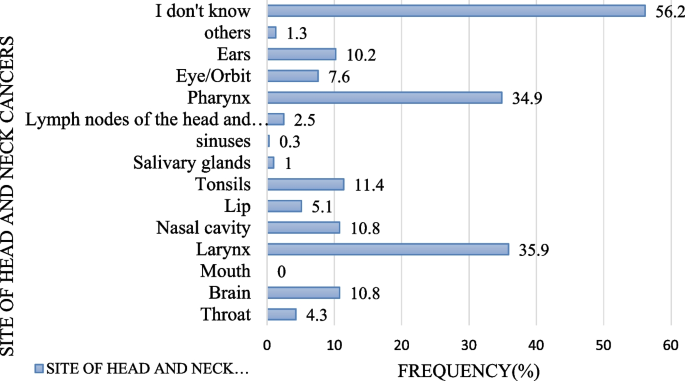
Majority of the respondents, 177(56.2%) didn’t knew anatomical sites of head and neck cancer and 4(1.3%) respondents incorrectly identified others anatomical sites of HNCs (like lung, chest and heart). Similarly, 34(10.8%) respondents incorrectly identified brain as a subsite of HNCs, 113(35.9%) respondents correctly knew larynx as another subsite while sinuses (0.3%) were the least correctly known subsites of HNCs (Fig. 1).
Anatomical sites of head and neck cancers identified by respondents
In this study, 208(65.9%) respondents didn’t know signs and symptoms of head and neck cancer and 9(2.8%) respondents incorrectly identified other nonspecific symptoms for HNCs (like chronic cough, blood in sputum, difficulty in breathing, loss of appetite, fever, persistent headache and poor vision). In the same study, neck mass was the most correctly identified symptom for HNCs, 92 (29.2%) while loosening of teeth was unknown to all respondents (Fig. 2).

Signs and symptoms of head and neck cancers identified by respondents
Majority of the respondents, 232(73.7%) knew cigarette smoking as a risk factor for head and neck cancer. Alcohol consumption was the second most commonly known risk factor, 205(65.1%). Similarly, 6(1.8%) respondents reported others risk factors for HNCs (like exposure to any chemical, drug abuse, multiple sexual partners and exposure to sugar containing foods) and 83(26.3%) respondents didn’t knew the risk factors for HNCs (Fig. 3).

Risk factors for head and neck cancers identified by respondents
The study has found that, 259(82.2%) respondents knew head and neck cancer to be potentially curable if diagnosed at early stages. Regarding vaccines, majority of the respondents were uncertain about its uses in preventing HNCs, 273(86.7%).
Majority of the respondents, 289(91.7%) knew surgery as the treatment option for head and neck cancer and the least known treatment option was immunotherapy, 5(1.6%). In the same study, 20(6.3%) thought cancer to have no treatment.
Majority of the respondents, 237(75.2%) knew cessation of cigarette smoking to be a preventive measure for head and neck cancer. Cessation of alcohol consumption was the second most commonly known preventive measure for HNCs, 213(67.6%) while use of fruits and vegetable was the least known preventive measure, 1(0.3%). In the same study, 77(24.4%) respondents didn’t know preventive measures for HNCs (Fig. 4).

Preventive measures for head and neck cancers identified by respondents
Association between socio-demographic characteristics of the respondents and correctly identified alcohol consumption as a risk factor for head and neck cancer
This study has found a significant association between correctly identified alcohol consumption as a risk factor for head and neck cancer and some socio-demographic characteristics of the study participants like gender, level of education and marital status (their corresponding p-values being less than 0.05). In the same study, no association was found between correctly identified alcohol consumption as a risk factor for head and neck cancer and respondent’s age (p value = 0.826) (Table 4).
Association between socio-demographic characteristics of respondents and correctly identified cigarette smoking as a risk factor for head and neck cancer
The study has found a statistically significant association between correctly identified cigarette smoking as a risk factor for head and neck cancer and some of the socio-demographic characteristics of the respondents (like gender, level of education and marital status) since all their corresponding p-values are less than 0.05 though no association was found between correctly identified cigarette smoking as a risk factor for head and neck cancer and respondent’s age (p value = 0.826) (Table 4).
Association between socio-demographic characteristics of respondents and correctly identified chewing/sniffing tobacco as a risk factor for head and neck cancer
The study has found a statistically significant association between correctly identified chewing/sniffing tobacco as a risk factor for head and neck cancer and some of the socio-demographic characteristics of the respondents (like gender, level of education and marital status) since their corresponding p-values are less than 0.05 though no association was found between correctly identified chewing/sniffing tobacco as a risk factor for head and neck cancer and respondent’s age (p value = 0.826) (Table 4).
Association between respondent’s risk factor status and correctly identified risk factor for head and neck cancer
The study has found no statistically significant association between respondent’s tobacco use/smoking status and correctly identified tobacco use/smoking as a risk factor for head and neck cancer (p value = 0.064). In the same study, a statistically significant association between respondent’s alcohol consumption status and correctly identified alcohol consumption as a risk factor for head and neck cancer was found (p-values = 0.07) (Table 5).