
Cardiovascular
Interventional echocardiography expected to grow thanks to new structural heart procedures
Aug
“We are moving to the right side of the heart where we now have transcatheter tricuspid valve repair and replacement (TTVR) devices. Ultimately, if I were to predict, I think that will be an easier market than the mitral anatomy, because the right ventricle is more accommodating in terms of its anatomical relationships with other competing structures,” Little explained.
Other experts in the structural heart space have echoed this comment and said tricuspid interventions will be the next big leap forward. They expect market clearance of new tricuspid devices will come before new mitral devices, which have been hampered by the very complex mitral anatomy.
More advanced training is needed for interventional echocardiographers
Little said the subspeciality of interventional echo developed slowly over the past 20 years to develop experts that can work with the heart team to guide transcatheter procedures. The field began to grow steadily after the FDA clearance of the first transcatheter aortic valve replacement (TAVR) device in 2012 and later approvals for MitraClip and left atrial appendage occlusion (LAAO) devices.
He said there is a lot on interest in this new subspecialty, but it is more involved than most people realize.
“You have to understand the catheters, the wires and the devices that are coming in to repair or replace. You have to be a person who understands conversations for the imaging and the intervention sides. You have to understand the tempo and the conversations in the procedure, the steps of the procedure and you need to provide the imaging. You have to bring together the procedure and imaging so they talk to each other in a way that probably nobody else in the room does. That’s really the speciality,” Little explained.
He said it is essential to “learn the dance and the rhythm” of the case and know when to step forward.
“You need to know when to watch, when to speak up and when should your voice be the loudest. These are things that are difficult to just put on a slide and tell somebody,” Little said.
This level of understanding requires an apprenticeship with an experienced interventional echocardiographer, he added. Learning all of these things also takes time.
Most of the echocardiographers that were the pioneers in this space at their centers are now being joined by new trainees who are just starting out in the field. Little said this has led to two distinct groups of interventional echocardiographers with very different different experience levels.
“This really speaks to the need for training, where the older group needs to train the newer group so we can have a mentor-mentee relationship. And now ASE just launched the first training guidelines for interventional echo where we list what are the competencies,” he said.
Procedure guidance needed for new type of transcatheter surgery
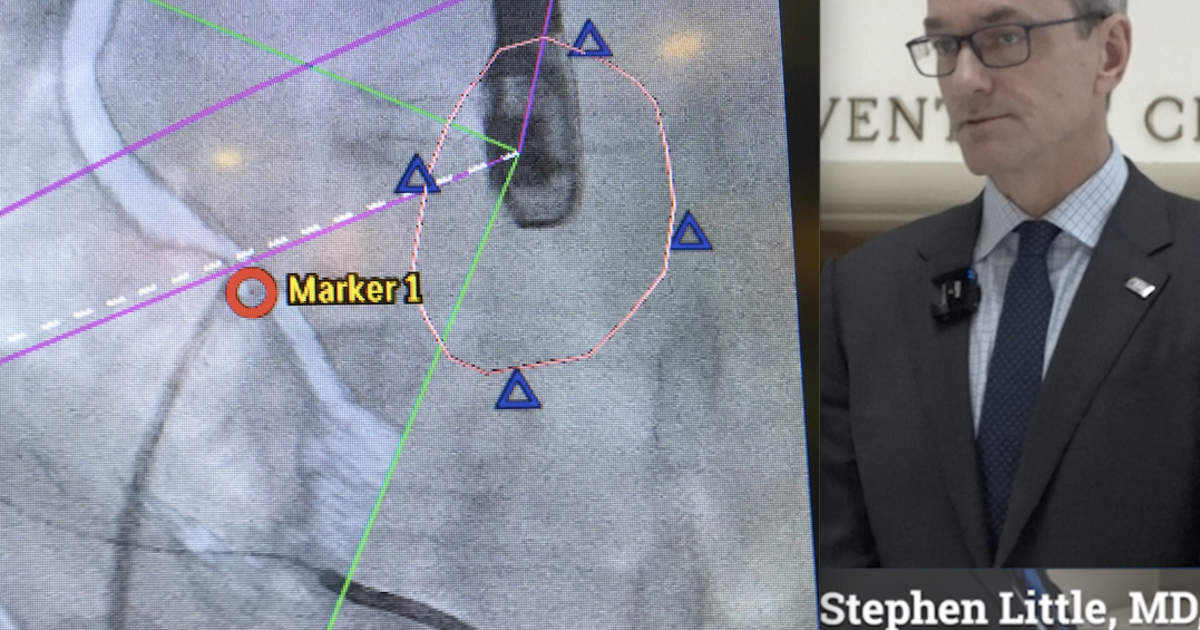
In the developing area of transcatheter mitral valve replacement (TMVR), a sizable number of patients may be excluded from the therapy because the valve hangs too far into the left ventricular outflow tract (LVOT), causing obstruction. New techniques have been developed to use an electrocautery wire to slice the native valve leaflets or a section of septal tissue to make room for the TMVR or TAVR devices. This precision cutting of soft tissue is guided by TEE. This procedure is also being investigated for use in hypertrophic cardiomyopathy (HCM).
“Increasingly you have to understand the tissues, because increasingly there are procedures to split the mitral valve, aortic valve or the ventricular septum,” Little explained. “The frontier is incredible and is changing very quickly.”