
Cancer and neoplasms
Overall Survival After Mohs Surgery for Early-Stage Merkel Cell Carcinoma
Aug
Key Points
Question
How does surgical approach affect long-term patient survival after excision of pathologically confirmed, localized, early-stage Merkel cell carcinoma (MCC)?
Findings
In this national cohort study of 2313 adults, excision of pathologically confirmed, localized, early-stage MCC with Mohs micrographic surgery was associated with significantly improved overall survival compared with wide local excision.
Meaning
These data suggest that, for early-stage MCC with pathologically confirmed negative regional lymph node disease, use of Mohs micrographic surgery vs conventional wide local excision as the primary surgical modality may lead to improved patient survival.
Importance
Merkel cell carcinoma (MCC) is a rare cutaneous malignant neoplasm with increasing incidence and high mortality. Although it is accepted that the optimal treatment for localized tumors is surgical, the data surrounding the optimal surgical approach are mixed, and current National Comprehensive Cancer Network guidelines state that Mohs micrographic surgery (MMS) and wide local excision (WLE) can both be used. The current National Comprehensive Cancer Network guidelines do not advocate a preference for MMS or WLE and suggest that they can be used interchangeably.
Objective
To evaluate the association of surgical approach with overall survival after excision of localized T1/T2 MCC.
Design, Setting, and Participants
This retrospective cohort study used the National Cancer Database to assess adults with T1/T2 MCC who were diagnosed between January 1, 2004, and December 31, 2018, with pathologically confirmed, negative regional lymph nodes and treated with surgery. The National Cancer Database includes all reportable cases from Commission on Cancer–accredited facilities. Data analysis was performed from October 2022 to May 2023.
Exposure
Surgical approach.
Main Outcomes and Measures
Overall survival.
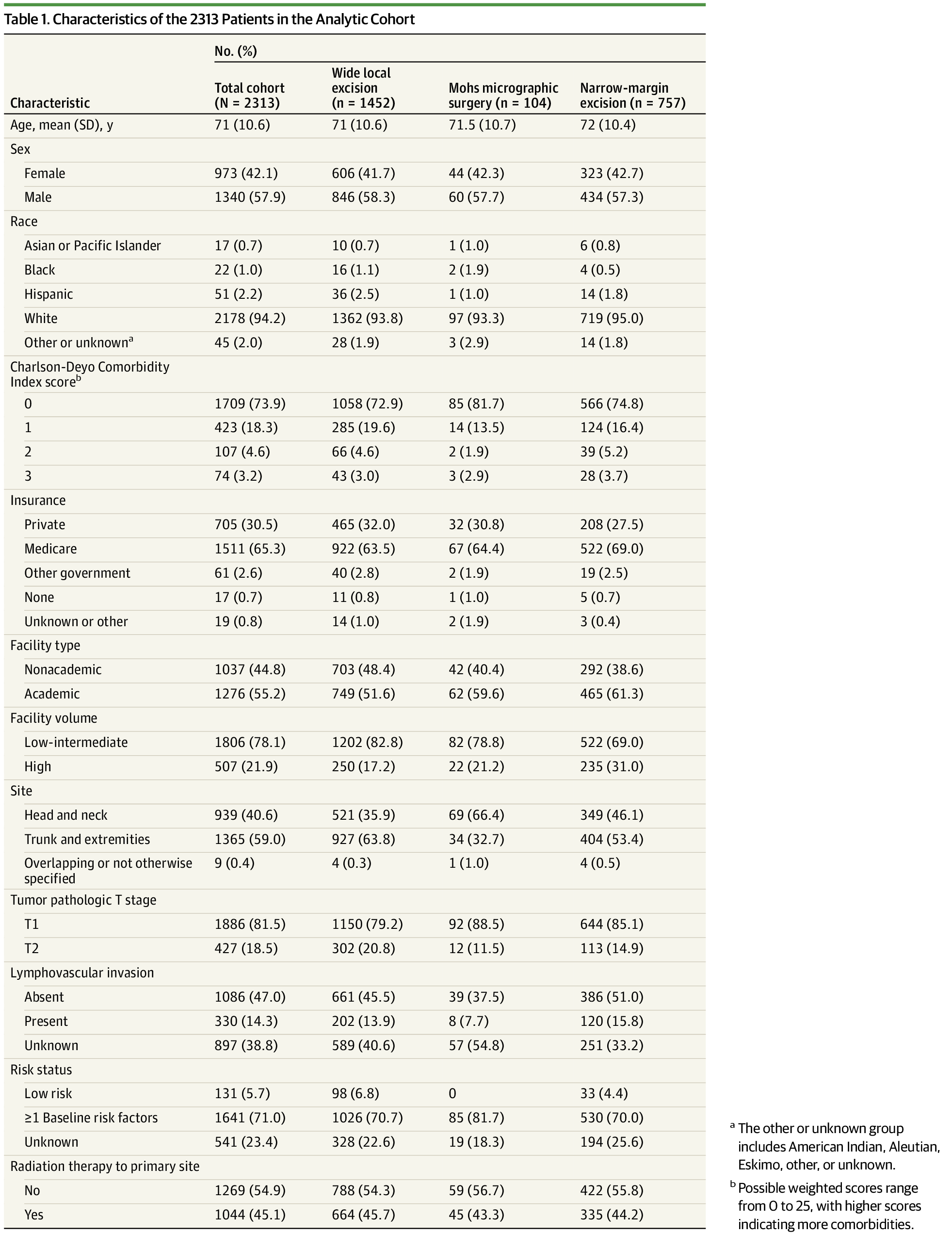
Results
A total of 2313 patients (mean [SD] age, 71 [10.6] years; 1340 [57.9%] male) were included in the study. Excision with MMS had the best unadjusted survival, with mean (SE) survival rates of 87.4% (3.4%) at 3 years, 84.5% (3.9%) at 5 years, and 81.8% (4.6%) at 10 years vs 86.1% (0.9%) at 3 years, 76.9% (1.2%) at 5 years, and 60.9% (2.0%) at 10 years for patients treated with WLE. Patients treated with narrow-margin excision had similar survival as those treated with WLE, with mean (SE) survival rates of 84.8% (1.4%) at 3 years, 78.3% (1.7%) at 5 years, and 60.8% (3.6%) at 10 years. On multivariable survival analysis, excision with MMS was associated with significantly improved survival compared with WLE (hazard ratio, 0.59; 95% CI, 0.36-0.97; P = .04). High-volume MCC centers were significantly more likely to use MMS over WLE compared with other centers (odds ratio, 1.99; 95% CI, 1.63-2.44; P < .001).
Conclusions and Relevance
In this cohort study, the use of MMS (compared with WLE) was associated with significantly improved survival for patients with localized MCC with pathologically confirmed negative lymph nodes treated with surgery. These data suggest that Mohs surgery may provide a more effective treatment for MCC primary tumors than conventional WLE, although the lack of randomization and potential for selection bias in this study highlight the need for future prospective work evaluating this issue.