
Infection
Congenital syphilis rates are soaring, but resources to stem infections are lacking
Sep
States are seeing an alarming surge in cases of congenital syphilis, a preventable infection that can lead to miscarriage, stillbirth, newborn death — or lifelong complications such as blindness or deafness.
Congenital syphilis, which occurs when a pregnant mother infected with the sexually transmitted infection syphilis passes it on to her fetus, disproportionately affects Black and Indigenous babies. It has seen a steady rise over the past decade, and during the pandemic between 2020 and 2021, cases rose 32%, from 2,157 to 2,855, according to the federal Centers for Disease Control and Prevention.
That’s about eight times the 358 babies born with the infection in 2011.
Across the nation, the congenital syphilis rate was highest in states in the South and Southwest. In 2021, Arizona had the highest rate, at about 232 cases per 100,000 births, followed by New Mexico (205), Louisiana (191), Mississippi (182) and Texas (182).
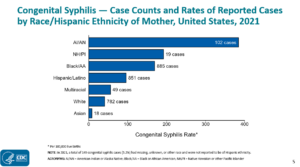
Nationwide in 2021, 102 babies born to American Indian and Alaska Native mothers had congenital syphilis — giving that group the highest rate, at about 385 per 100,000 births, followed by 29 Native Hawaiian and Pacific Islander babies, at a rate of 192 per 100,000.
Babies born to Black mothers had the highest number of overall cases, 885, or nearly 170 per 100,000 births, and those born to Hispanic or Latino mothers saw a rate of 96 per 100,000 births. There were 782 cases of babies with congenital syphilis born to white mothers, about 41 per 100,000 births.
While the CDC hasn’t yet released official figures for last year’s cases, a study on Mississippi released last week in the agency’s journal Emerging Infectious Diseases found a 1,000% surge in the state — from 10 cases in 2016 to 110 last year.
Experts say a confluence of factors are at play in the rise and the disparities, including poverty, stigma, a lack of access to prenatal care, drug use, a need for more medical education and screenings, and a lack of funding for public health efforts.
Irreversible complications
Syphilis is a sexually transmitted infection that, if left untreated, can cause serious health problems, including brain and nerve issues as well as blindness.
An infected pregnant mother can pass syphilis on to her fetus. Babies born with congenital syphilis who aren’t treated within the first three months of life are more likely to suffer irreversible complications such as deafness or blindness, according to the CDC. Nearly 40% can be stillborn or die as a newborn.
Parents might not know they have syphilis, as it can occur with mild or no symptoms. Babies can also be born without symptoms or develop skin rashes, jaundice, bone damage, anemia, enlarged organs or meningitis. Syphilis is treatable with antibiotics such as penicillin, though drugmaker Pfizer recently warned of a looming shortage of its medication for the disease into next year.
This is absolutely preventable. What we need are the resources.
– Dr. Daniel Edney, Mississippi’s state health officer
The steady reemergence of the treatable disease mainly points to failures in public health systems, said Dr. Daniel Edney, state health officer of the Mississippi State Department of Health and an internal medicine physician.
“Syphilis has not thrown us a curveball. Syphilis is doing what syphilis has done for thousands of years, and the treatment has not changed,” he said. “This is absolutely preventable. What we need are the resources.”
Missed screenings of asymptomatic babies can inhibit intervention and can cause permanent disabilities. Blindness and deafness can take a couple of months to a couple of years to manifest, said Dr. Charlotte Hobbs, a pediatrician and infectious disease specialist at the University of Mississippi Medical Center.
“We’ve had cases of babies who have fallen through the cracks, and by the time we see them, even in a couple of months of age, they are neurologically devastated,” Hobbs said.
It wasn’t until March that the Mississippi State Department of Health began mandating screenings during the first and third trimesters of pregnancy, and during labor if the patient has no previous documentation of syphilis testing.
More Babies Are Being Born With Syphilis. Blame Meth and Opioids.
Seven other states, according to a 2021 CDC analysis, don’t mandate testing at any point during pregnancy. Just 18 states plus Washington, D.C., require third trimester screening, with five of those requiring it only if there’s high risk. Only a dozen states require screening during delivery, with seven of them requiring it only if there is increased risk.
But to stem the soaring rates, experts such as Houston-based obstetrician and gynecologist Dr. Irene Stafford say clinicians need to move past relying on these mandates: Health professionals should screen everyone wherever they show up for care, whether they seem at risk or not, if they have the possibility of becoming pregnant or getting someone pregnant, she said.
“It’s screening at any opportunity, instead of siphoning it into just a prenatal visit,” said Stafford, an associate professor at UTHealth Houston McGovern Medical School. Texas had 680 cases in 2021.
“Not everybody has prenatal care,” she said. “Not everybody gets access to prenatal care quickly — especially the underserved minority population.”
A lack of access
Rural communities in the South and Western states have large populations of Black, Hispanic and Indigenous people whose maternal health care has vanished as rural hospitals and clinics shutter. It’s well documented that people lacking a medical doctor or transportation may instead visit emergency rooms for care, so clinicians should increase testing there, Stafford said.
The pandemic disrupted testing and well-woman visits, but the nation hit a 20-year high in congenital syphilis cases in 2018, before the pandemic.
In Mississippi, the increase was likely not exacerbated much by the pandemic, said Dr. Thomas Dobbs, an expert on sexually transmitted infections and dean of the School of Population Health at the University of Mississippi.
“Services have been moving out of health departments for many years, with cutbacks in our public health infrastructure,” said Dobbs, a former Mississippi state health officer and co-author of last week’s study.
‘Shocking’ Rise in STIs During COVID Alarms Health Workers
Edney, of the Mississippi State Department of Health, noted that the state last year rejected a request from his department to hire 100 public health nurses to help rebuild a slashed workforce.
Edney said his agency has experienced “a drastic reduction in funding,” including a significant cut to a workforce tasked with fighting syphilis and other sexually transmitted infections. These are field epidemiologists that the National Coalition of STD Directors calls the “heart and soul” of prevention.
“I’m just having to cannibalize funds everywhere I can to invest into this space so we can get our arms around the whole syphilis problem, which spills over into pregnancy that generates the congenital syphilis cases,” Edney said.
In Mississippi, half of counties are so-called maternity care deserts, or counties without any obstetric centers or maternal health care clinicians. Mississippi also ranks in the bottom 10 states in per capita state public health funding at $16 per resident, according to the University of Minnesota State Health Access Data Assistance Center.
Getty Israel, founder of the nonprofit women’s health clinic Sisters in Birth in Jackson, Mississippi, said a long-standing barrier for her community-level work is lack of funding and willingness from Mississippi agencies to partner with her on-the-ground team.
“We do the best we can with our community health workforce. We don’t have the funding that hospitals have,” she said.
Stigma, social factors
Stigma, shame, fear of racism and judgment can hinder patients’ open communication with clinicians, says family nurse practitioner Natassia Williamson in Glendale, Arizona. The state saw the highest congenital syphilis rate in the nation in 2021, as well as a 449% syphilis increase among women since 2015, according to the state.
“I’ve had patients who, when they come to see me … [say], ‘I don’t want to see that provider because I think that they’re just mean,’ or they think they might be racist,” said Williamson, who has worked in tribal clinics.
Underscoring racial disparities in cases, syphilis is also a highly stigmatized disease with roots in medical violations toward Black people — notably, the federal Tuskegee syphilis study that withheld treatment from Black men for more than 40 years.
Williamson said providers need to be deliberate about cultivating trust. Research has also shown a higher risk of intimate partner violence at play.
“One of the main barriers is the trust in the system,” she said. “If they confide in you that they have a background where they’re at risk, be compassionate, and just treat them how you would want someone to treat you if you were in that situation.”
Community health workers are also key to fighting the spread, Israel said. That includes disease intervention specialists who are trained to provide non-judgmental sexual health education.
Infections are disproportionately high in men who have sex with men, who — along with men who have sex with men and women — made up more than a third of the 53,000 cases of primary- and secondary-stage syphilis in 2021.
“We’re not tracking partners like we used to. There’s not that infrastructure,” said Dobbs, who added that STI testing is increasingly moving from public health clinics to private health clinics, limiting testing access for disadvantaged patients. Arizona spends less per capita on public health — $15 — than any other state.
Dr. Veronica Gillispie-Bell, an OB-GYN and medical director at New Orleans-based Ochsner Health and the Louisiana Perinatal Quality Collaborative, said men lack regular checkups for STDs.
Unlike well-woman appointments, “Guys don’t have anything like that. They don’t have a ‘well-man’ exam that STD testing would be part of,” she said. “There isn’t a routine screening for men.”
SUPPORT NEWS YOU TRUST.