
Infection
Global burden of lower respiratory infections attributable to secondhand smoke among children under 5 years of age, 2010–2019: a systematic analysis of the global burden of disease study 2019
Oct
Global level
In 2019, 6.94% (3.80–10.12%) of under-5 LRIs deaths were attributable to SHS globally, with an under-5 mortality rate of 7.02 per 100,000, a decrease of 5.77% since 2010. In addition, 6.95% (3.81–10.13%) of under-5 LRIs DALYs were due to SHS, with a rate in under-5s of 619.36 DALYs per 100,000, a 5.77% decrease since 2010 (Table 1).
Regional level
In 2019, Oceania, Central Asia, and South Asia had the highest under-5 mortality rates (27.53 for Oceania, 16.60 for Central Asia, 11.18 for South Asia) and DALY rates (2,421.89 for Oceania, 1,461.52 for Central Asia, 987.25 for South Asia) from LRIs attribute to SHS, with the lowest rates in under-5s of mortality and DALYs in Western Europe (mortality rate: 0.19, DALYs rate: 17.55), Australasia (mortality rate: 0.24, DALYs rate: 21.55), and high-income North America (mortality rate: 0.35, DALYs rate: 31.45) (Table 1). From 2010 to 2019, all regions showed a decrease in the under-5 mortality rates from LRIs attributed to SHS, with the largest decreases in East Asia (− 9.72%), Central Sub-Saharan Africa (− 9.07%), and Eastern Europe (− 7.44%) (Table 1). The DALY rates in under-5s also decreased in all regions from 2010 to 2019, with the largest decreases also in East Asia (− 9.70%), Central Sub-Saharan Africa (− 9.05%), and Eastern Europe (− 7.40%).
The percentage of deaths and DALYs caused by LRIs attributable to SHS slightly decreased or even remained stagnant from 2010 to 2019 globally among children under 5 years old. This pattern was observed in most regions, with the exception of Andean Latin America, the Caribbean, high-income North America, Oceania, South Asia, Southeast Asia, Tropical Latin America, and Western Sub-Saharan Africa, for which percentages were slightly increased from 2010 to 2019. Noticeably, SHS was attributed to a large extent of the under-5 LRIs burden in Eastern Europe (20.78%), East Asia (19.59%), and Central Europe (18.16%) in 2019.
National level
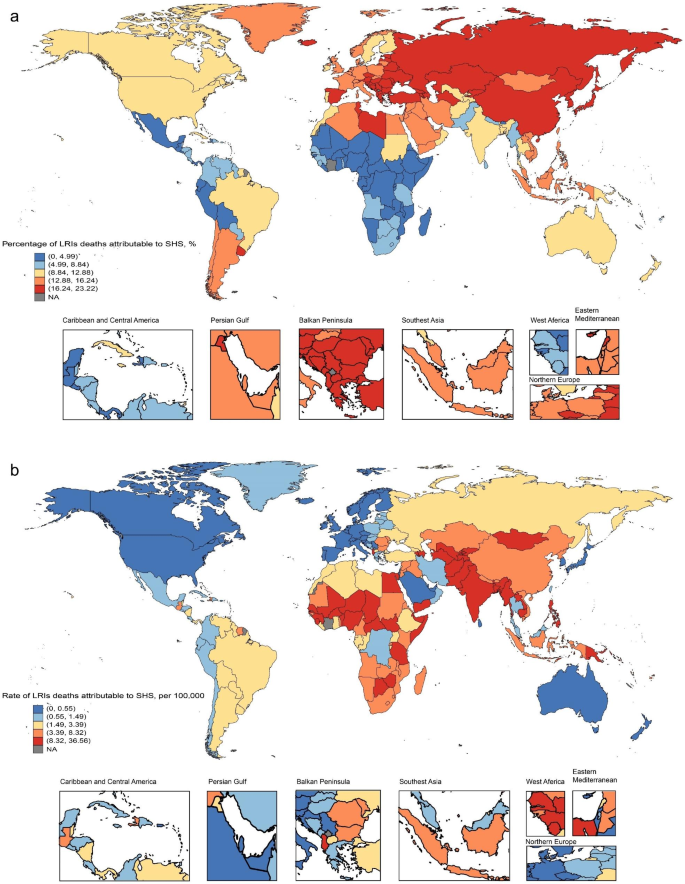
In 2019, the national under-5 mortality rates for LRIs varied from 0.05 to 36.56 per 100,000. The highest rates were seen in Azerbaijan (36.56), Turkmenistan (32.90), and Papua New Guinea (32.24), whereas the lowest rates were found in Finland (0.05), Norway (0.07), and Sweden (0.09) (Fig. 1B, Table S1). In 2019, the national DALY rate in under-5s of LRIs ranged from 7.66 to 5838.06 patients per 100,000. The highest rates were also seen in Azerbaijan (3224.34), Turkmenistan (2890.91), and Papua New Guinea (2836.02), whereas the lowest rates were in Finland (5.39), Norway (7.37), and Sweden (9.25) (Figure S1B, Table S1). The percentage change in the under-5 mortality rate, from 2010 to 2019, differed noticeably between countries, with Iran (Islamic Republic of) (16.09%), Saudi Arabia (11.04%), and Cook Islands (10.57%) having the largest decreases. In contrast, the Northern Mariana Islands (2.79%), Dominica (2.71%), Burkina Faso (0.32%), Ukraine (0.14%), and Niger (0.06%) had increasing trends (Table S1). Over the same period, Iran (Islamic Republic of) (16.03%), Saudi Arabia (10.66%), and Cook Islands (10.50%) had the largest decreases in the DLAYs rate, whereas increases were also found in the Northern Mariana Islands (2.81%), Dominica (2.72%), Burkina Faso (0.32%), Ukraine (0.16%), and Niger (0.07%). In 2019, Bosnia and Herzegovina (23.22%), Armenia (23.12%), and Montenegro (23.07%) showed the highest percentage of LRIs burden due to SHS, whereas Sao Tome and Principe (1.33%), Ethiopia (1.35%), and the Democratic Republic of the Congo (1.37%) showed distinctly small extent of this burden (Fig. 1A, Figure S1A, Table S1).
Global burden of LRIs deaths attributable to SHS among children under 5 years of age in 2019. (a) Percentage of LRIs deaths attributable to SHS; (b) Rate of LRIs deaths attributable to SHS. LRIs: lower respiratory infections; SHS: secondhand smoke
Age-sex pattern and temporal trend
Globally, we observed slight decreases in the PAF of DALYs from 2010 to 2019 (Fig. 2A), and the PAF was higher in children < 1 year than in children 1–4 years (Fig. 2B C). This pattern was observed for most regions, with the exception of South Asia and Sub − Saharan Africa, for which PAF were slightly increased after 2010. With regard to the time trend in the DALYs rate of LRIs attributable to SHS, we found a decrease in most super-regions from 2010 to 2019, whereas the rate of DALYs were stagnant and remained at the lowest level over time in high − income regions. The rate of DALYs is much greater in children younger than 1 year than in children aged 1–4 years. The highest rate of DALYs among children under 1 year of age was observed in South Asia, while the highest rate of DALYs among children aged 1–4 years was shown in Sub-Saharan Africa. With the exception of South Asia, which shows a higher DALYs rate in females, other regions show a similar pattern of the LRIs burden attributable to SHS between females and males (Fig. 2D and E). Regardless of age-sex pattern or time period, the PAFs and rates for DALYs in Latin America and Caribbean are lower than global levels. However, in high-income regions, PAF levels are remarkably above global levels despite low rates of DALYs in under-5s (Fig. 2A).

Temporal trend in LRIs DALYs attributable to SHS among children under 5 years of age, 2010–2019. (a) Data are for all ages and both sexes by GBD super-region and globally; (b) Data are for male; (c) Data are for female; (d) Data are for < 1 year old; (e) Data are for 1–5 years old. LRIs: lower respiratory infections; SHS: secondhand smoke; DALYs: disability-adjusted life-years; PAF: population attributable fraction
Association with the SDI
At the regional level, we found a negative association between the SDI and the DALYs rate of LRIs in uner-5s from 2010 to 2019 (Fig. 3), as well as the SDI and mortality rate (Figure S2). Except for some regions with high SDI, such as Australasia, Western Europe and high-income Asia Pacific, where the under-5 mortality and DALYs rate remained stable, low- and middle-SDI countries showed large decreases in the rate of mortality and DALYs from 2010 to 2019 with the development of SDI. Oceania and Central Asia had higher level than the other regions based on their SDIs, from 2010 to 2019 (Fig. 3A, Figure S2A). At the country level, in 2019, the burden of LRIs decreased with increasing socioeconomic development up to SDI. Countries and territories such as Azerbaijan, Turkmenistan, Papua New Guinea, and Cambodia had much higher than expected burdens, whereas Burundi, Liberia, Ethiopia, and the Democratic Republic of the Congo had much lower than expected burdens (Fig. 3B, Figure S2B).

The correlation between SDI and DALYs rate of LRIs attributable to SHS among children under 5 years of age, 2010–2019. (a) In 21 GBD regions and five SDI regions; (b) In 204 countries and territories. SDI: sociodemographic index; DALYs: disability-adjusted life-years; LRIs: lower respiratory infections; SHS: secondhand smoke