
Infection
Invasive Histoplasmosis Presenting as Tenosynovitis in an Immunocompromised Patient
Nov
FINAL DIAGNOSIS
Histoplasma tenosynovitis
HISTORY OF PRESENT ILLNESS
A 40-year-old man with medical history of long-standing systemic lupus erythematosus complicated by lupus nephritis proven by biopsy result presented with a 2-week history of right hand and arm edema, erythema, and tenderness. At that time, it was determined these signs and symptoms were likely due to a lupus flare. His home prednisone dose was increased from 15 to 40 mg orally daily, and mycophenolate mofetil (MMF) was later increased to 1000 mg orally twice daily, with clindamycin 600 mg orally 3 times daily for 2 weeks because of concern for concurrent cellulitis. Symptoms resolved. Eight months later, he presented with 3 weeks of increasing pain and edema of his right hand with no antecedent trauma, no fevers, no chills, and no night sweats.
MEDICAL HISTORY
He has a history of systemic lupus erythematosus, lupus nephritis, and cerebrovascular accident.
KEY MEDICATIONS
MMF 1000 mg orally twice daily
Prednisone 40 mg orally daily
EPIDEMIOLOGICAL HISTORY
He works as a computer engineer at a local university. He is married and lives with his wife and son. He has not done domestic or international travel recently. He does not recall any insect bites. He owns a dog but has no pet fish, aquarium, or seawater exposure. He has no history of sexually transmitted diseases. He denies hiking or camping outdoors. He denies use of illegal drugs, cigarette smoking, and alcohol. His family history is unremarkable.
PHYSICAL EXAMINATION
The patient appeared well, not in cardiorespiratory distress but in mild pain. His blood pressure level was 130/80 mm Hg, heart rate was 86 beats per minute, temperature was 98 °F (36.7 °C), and respiration rate was 16 breaths per minute. His right hand and finger were edematous and erythematous and warm to touch, and he was unable to flex his finger because of pain. His right arm was edematous extending to his midarm, with erythema extending to his axilla with no lymphadenopathy. The remainder of the physical examination findings were normal.
STUDIES
White blood cell count was 7.42 K/μL (reference range, 4.4-11.3 K/μL), with polymorphonuclear leukocytes at 94%, lymphocytes at 2%, and monocytes at 3%. The hemoglobin level was 10 g/dL (reference range, 13.8-17.4 g/dL) and hematocrit level was 29.5% (reference range, 41%-51%). The platelet level was 179 K/μL (reference range, 150-450 K/μL). His creatinine level was 2 mg/dL (reference range, 0.6-1.3 mg/dL) and blood urea nitrogen level was 100 mg/dL (reference range, 7-20 mg/dL). His C-reactive protein (CRP) level was 34.2 mg/L (reference range, < 5 mg/L). Right hand and arm radiograph results were normal. Right hand MRI scan showed changes consistent with circumferential synovial proliferation/ thickening involving the second, third, and fourth flexor digitorum profundus and flexor digitorum superficialis tendons within the tendon sheath, favoring an inflammatory process.
CLINICAL COURSE
The patient underwent joint aspiration of the right index interphalangeal joint, where only extracellular monosodium urate crystals were seen. Intravenous methylprednisolone sodium succinate 60 mg daily was started for acute gout flare but yielded no significant improvement. CRP level continued to increase to 54 mg/L. The patient then underwent extensive debridement of volar and dorsal right index finger as well as arthrotomy and synovectomy of the right index proximal interphalangeal joint. Gram stains, fungal stains, and crystals yielded negative results. Tissue samples were also sent for pathology tests. He was discharged on prednisone 60 mg orally daily.
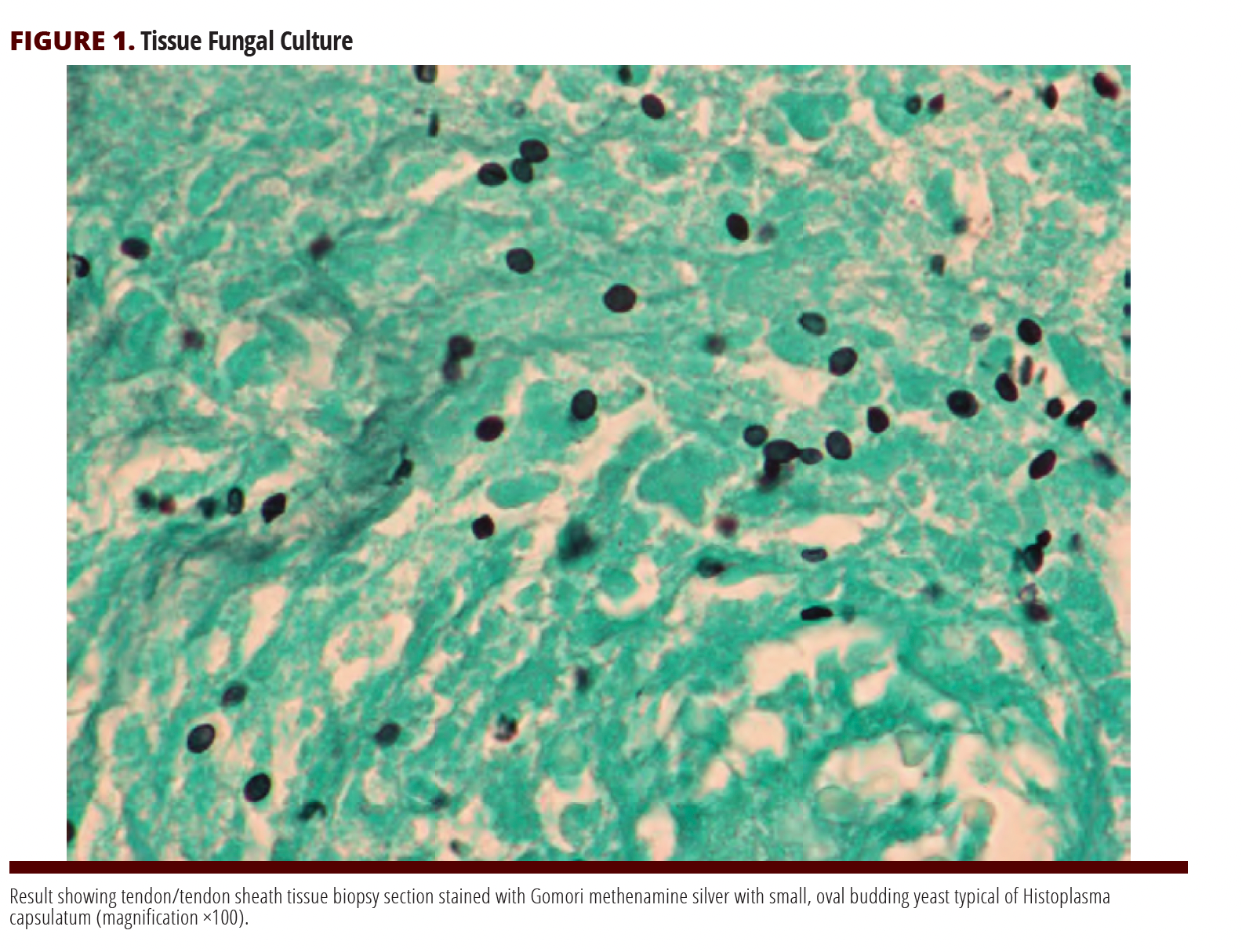
DIAGNOSTIC PROCEDURES AND RESULTS
After discharge, final pathology results revealed septate hyphae bearing round and pear-shaped tuberculate and knobby, thick-walled macroconidia consistent with Histoplasma capsulatum (FIGURES 1-3). Serum Histoplasma antibody mycelial complement fixation (CF) result was 1:16, and yeast CF result was 1:16. H capsulatum was identified by DNA probe (susceptibilities: amphotericin B at 0.06 μg/mL, itraconazole ≤ 0.03 μg/mL, and posaconazole ≤ 0.03 μg/mL).
TREATMENT AND FOLLOW-UP
The patient was started on oral itraconazole 200 mg 3 times daily for 3 days as loading dose. This was decreased to 200 mg twice daily as maintenance, with therapeutic itraconazole levels demonstrated. He has been maintained on this regimen as a long-term suppression therapy while taking MMF and prednisone. No reactivations were noted on future outpatient follow-up visits.

DISCUSSION
H capsulatum is an intracellular dimorphic fungus that causes respiratory and systemic infections in both immunocompetent and immunocompromised patients.1 The dimorphic characteristic of Histoplasma is dictated by the environment where it is isolated. It exists as mold in soil at a temperature of 20 to 25 °C.1 Histoplasma in this form appears as septate hyphae bearing round and pear-shaped tuberculate and knobby, thick-walled macroconidia. On the other hand, it appears as small, oval budding yeast in host tissues where the temperature is warmer (at approximately 37 °C).1 It is endemic to certain areas of North America, South America, Africa, and Asia, and there are some reports of it in Europe. In the United States, most cases are reported in the Ohio and Mississippi river valleys.2 Inhalation from aerosolized soil is the most common means of transmission and is usually exacerbated by activities that disrupt soils, particularly those rich in bird and bat excrement. This excrement enhances the growth of the organism by accelerating sporulation.2
Histoplasma tenosynovitis has been reported and is usually accompanied by bony involvement. Whether the original focus of infection is the bone or the tenosynovium is unclear because bone infection can precede the latter.3 In our patient, we used itraconazole, an azole antifungal that disrupts the fungal cell wall by interfering with chitin synthesis, as maintenance therapy.4 It distributes extensively to tissues such as bone, liver, sputum, adipose, and keratin.4
Cell-mediated immunity is vital to limiting the extent of histoplasmosis but does not eradicate it completely.2 Patients with defective or depressed cell-mediated immunity, either from a condition such as AIDS5 or from medications (eg, methotrexate6 and tumor necrosis factor inhibitors7), are at risk for reactivation. Our patient is taking prednisone and MMF, which act on cell-mediated immunity, suppressing the main mechanism of containment of H capsulatum. Corticosteroids decrease the response to antigens and mitogens by modulating different mechanisms in the proliferative cascade of lymphocytes, including direct effects on lymphocytes themselves.8 MMF can affect both T-cell and B-cell activity by depleting guanosine nucleotides and can therefore affect both cell-mediated and humoral immunity.9 Both agents played a role in reactivation in our patient.
Histoplasmosis is a common endemic fungal infection in patients with AIDS.10 In a prospective multicenter trial of itraconazole as maintenance therapy for histoplasmosis in patients with AIDS, once-daily dosing of 200 mg was highly effective in most patients,11 but relapses are common unless suppressive maintenance therapy is added. Most patients stay on antifungal therapy for life.5 However, it has been shown that discontinuation of antifungal therapy in patients with HIV on consistent antiretroviral therapy with sustained immunologic response is safe and a possible option in this population.12
In conclusion, patients who are immunocompromised, particularly those with impaired cell-mediated immunity, are at high risk for invasive and disseminated histoplasmosis, with high rates of recurrence. Treatment with itraconazole is effective, but long-term therapy may be needed if the immunosuppression is not corrected.

References
- Woods JP. Revisiting old friends: developments in understanding Histoplasma capsulatum pathogenesis. J Microbiol. 2016;54(3):265-276. doi:10.1007/s12275-016-6044-5
- Wheat LJ, Freifeld AG, Kleiman MB, et al; Infectious Diseases Society of America. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis. 2007;45(7):807-825. doi:10.1086/521259
- Care SB, Lacey SH. Recurrent histoplasmosis of the wrist: a case report. J Hand Surg Am. 1998 Nov;23(6):1112-1114. doi:10.1016/S0363-5023(98)80025-7
- Mangino JE, Pappas PG. Itraconazole for the treatment of histoplasmosis and blastomycosis. Int J Antimicrob Agents. 1995;5(4):219-225. doi:10.1016/0924-8579(95)00010-6
- Wheat LJ, Connolly-Stringfield PA, Baker RL, et al. Disseminated histoplasmosis in the acquired immune deficiency syndrome: clinical findings, diagnosis and treatment, and review of the literature. Medicine (Baltimore). 1990;69(6):361-374. doi:10.1097/00005792-199011000-00004
- Witty LA, Steiner F, Curfman M, Webb D, Wheat LJ. Disseminated histoplasmosis in patients receiving low-dose methotrexate therapy for psoriasis. Arch Dermatol. 1992;128(1):91-93.
- Jain VV, Evans T, Peterson MW. Reactivation histoplasmosis after treatment with anti-tumor necrosis factor alpha in a patient from a nonendemic area. Respir Med. 2006;100(7):1291-1293. doi:10.1016/j.rmed.2005.09.020
- Cohn LA. The influence of corticosteroids on host defense mechanisms. J Vet Intern Med. 1991;5(2):95-104. doi:10.1111/j.1939-1676.1991.tb00939
- Allison AC. Mechanisms of action of mycophenolate mofetil. Lupus. 2005;14(suppl 1):s2-s8. doi:10.1191/0961203305lu2109oa
- Wheat LJ, Chetchotisakd P, Williams B, Connolly P, Shutt K, Hajjeh R. Factors associated with severe manifestations of histoplasmosis in AIDS. Clin Infect Dis. 2000 June;30(6):877-81. doi:10.1086/313824
- Hecht FM, Wheat J, Korzun AH, et al. Itraconazole maintenance treatment for histoplasmosis in AIDS: a prospective, multicenter trial. J Acquir Immune Defic Syndr Hum Retrovirol. 1997;16(2):100-107. doi:10.1097/00042560-199710010-00005
- Goldman M, Zackin R, Fichtenbaum CJ, et al; AIDS Clinical Trials Group A5038 Study Group. Safety of discontinuation of maintenance therapy for disseminated histoplasmosis after immunologic response to antiretroviral therapy. Clin Infect Dis. 2004;38(10):1485-1489. doi:10.1086/420749