
Cardiovascular
Job stress, a source of hypertension among workers in Sub-Saharan Africa: a scoping review
Nov
Search results
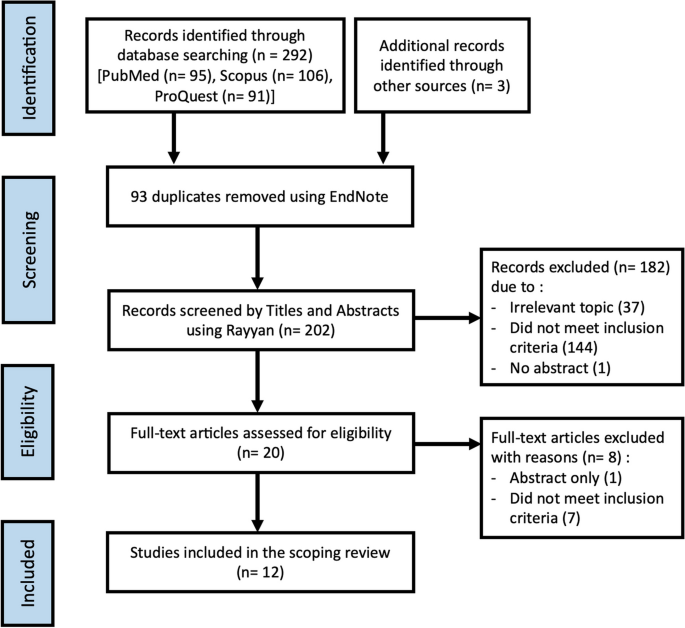
A total of 295 articles were identified, mainly in the three electronic databases and only 3 additional records were manually found. Moreover, 93 duplicate articles were removed, and the remaining 202 were screened according to the inclusion criteria. After a review of the title and abstracts, 20 articles were included for the full-text review. Furthermore, 8 articles were excluded during the full-text screening regarding the inclusion criteria. Finally, 12 articles fulfilled the inclusion criteria and were included in the current scoping review (Fig. 1).
PRISMA Flow Diagram for inclusion process of articles in the review
Type of studies and objectives
The 12 studies were published between 2003 and 2022. All studies employed quantitative measures. Of the studies included in the present scoping review, 8 were cross-sectional studies [31,32,33,34,35,36,37,38], and 3 case–control studies [39,40,41]. The design was not reported in a study, but the methodology followed was a cross-sectional study [42]. Regarding the geographical location of these studies, 3 were carried out in South Africa, 3 in the Democratic Republic of Congo, 2 in Nigeria, 1 in Benin, 1 in Cameroon, 1 in Congo, and 1 in Sudan. The geographical distribution of these studies is presented in the Fig. 2.

Hypertension and job stress: published articles in Sub-Saharan Africa
The objective of several studies was to determine the prevalence of HTN and associated factors in the workplace [33,34,35, 37]. Others investigated the relationship between job stress and HTN [39, 40] and another sought to determine the prevalence of HTN and other cardiovascular risk factors among workers [36].
Quality appraisal
Of the 12 included articles, 3 were high-quality [32, 37, 38], 6 were medium-quality [31, 33,34,35, 39, 41], and 3 were low-quality [36, 40, 42] according to the Joanna Briggs Institute (JBI) critical appraisal tools used, providing a general overview of the quality of these studies (Additional file 2).
Narrative analysis
The summary of study characteristics and findings of the included articles is presented in Table 1.
Study participants
The sample size of included studies ranged between 84 participants in the Democratic Republic of Congo [39] and 21,307 participants in South Africa [31]. The ages of the subjects ranged from 18 to 79 years. However, 4 of these studies did not report the age range [32,33,34, 39]. All the studies included both male and female participants.
Measurement of exposure
Job stress measurement was performed in 9 studies [31,32,33, 35, 37, 38, 40,41,42]. The most widely used stress assessment model is the Karasek model in 5 studies with the 26-item version. The “Job strain” was defined by a psychological demand of less than 21 and a decision latitude of less than 71 [35, 37, 38, 40, 41]. Although, only one study did not describe how stress was assessed following this model [41].
In addition to that exposure measurement, the measurement of blood pressure (BP) was done in 10 studies [32,33,34,35,36,37,38,39,40,41]. HTN was defined as SBP ⩾140 mmHg and by DBP ⩾90 mmHg. Nevertheless, 2 studies did not report how HTN was defined [33, 40]. Only 6 reported the measurement of both job stress exposure and blood pressure.
Activity sectors covered by the included studies
Four studies were carried out in the health sector [33, 38, 39, 42], 2 in the banking sector [34, 36], 2 in the education sector [31, 41], 2 in the industry sector [37, 40], 1 in the administration sector [35] and 1 multi-sector worker study among blue-collar workers (mining, manufacturing, and construction) and white-collar workers (banking, IT, and retail companies) [32].
Prevalence of hypertension and job stress
The prevalence of HTN ranged from 14.3% [40] to 45.9% [34]. A high proportion of hypertensive participants (35.4% to 70.6%) were unaware that they had HTN at the time of the study [33,34,35, 37]. A study highlighted that blood pressure was higher in males than in females [36]. The prevalence of job stress ranged from 16.6% [42] to 47.9% [37]. The stress level was related to occupation and among these most stressed subjects, we also had the highest number of hypertensives [32, 39, 40]. This stress level was also highlighted higher in males than in females [31, 38].
Association between hypertension and job stress
In total, 9 studies reported a relationship between HTN and job stress [31, 34,35,36,37,38,39,40, 42]. These studies noted that an increase in a job stress situation was associated with an increase in blood pressure. The perceived stress among workers was positively associated with HTN (r = 0.17, p < 0.05) [42]. Of the studies that reported an association between HTN and job stress, only 2 studies adjusted for other factors. Thus, after adjustment, job stress (OR = 2.4 [1.5–4.4], p < 0.001) was significantly associated with HTN in the first study [37], and in the second, that was statistically significant only in men (OR = 1.12 [1.06–1.20], p < 0.001) [31].
Other factors known as traditional risk factors of HTN have been reported as associated with HTN, such as age [33, 34, 37]; gender where males were more likely to be affected by HTN (OR = 1.12 [1.06–1.20]) [31], (OR = 2.2 [1.3—3.7]) [37]; heredity or family history of HTN (OR = 2.4 [1.3—4.7]) [37], also highlighted by Khaild et al. [34] and Adjobimey et al. [35]; overweight (OR = 2.9 [1.4—6.1]) or obesity (OR = 4.3 [1.9—9.8]) [37] that were also identified in other studies [33,34,35]; alcohol consumption (OR = 7.0 [2.36–20.70]) [39], reported as well in 2 studies [31, 36]; smoking [31, 34, 36, 39]; physical activity (OR = 2.3 [1.2—4.3]) [37], (r = -0.193, p = 0.001) [33], found also in other studies [34, 36].
Stress management and health promotion program in the workplace
None of the studies documented the availability of a workplace health promotion program, particularly concerning cardiovascular disease risk factors. However, a study that assessed stress management among healthcare workers in hospitals noted that HTN was inversely associated with stress management (r = -0.14, p < 0.05) [42]. Nevertheless, this evaluation did not mention a specific job stress management program implemented in these hospitals. The authors suggest that effective lifestyle and health promotion programs are needed to reduce stress and health risks for healthcare workers.