
Blood
Not all major trauma patients benefit from receiving additional blood-clotting factors when treating blood loss: Study
Oct
The Centre for Trauma Sciences, based at Queen Mary University of London, aims to reduce deaths from severe bleeding after major trauma.
The CRYOSTAT-2 trial is the largest ever trial conducted in seriously bleeding trauma patients. The trial, a collaboration between the Centre for Trauma Sciences and the NHS Blood and Transplant Clinical Trials Unit, investigated whether giving bleeding major trauma patients additional blood-clotting factors as soon as they were admitted to hospital, rather than later in the process (as is current practice), would improve survival rates.
Having originally identified that trauma patients develop a severe clotting disorder, the Centre subsequently found that a central component of this was loss of fibrinogen—which is the fundamental protein required to form blood clots. When fibrinogen levels are identified as being low, trauma patients are given fibrinogen concentrates to help bring their levels back to normal and support coagulation.
In the earlier CRYOSTAT study, researchers found that they could quickly give all bleeding trauma patients a large dose of fibrinogen (as the blood component cryoprecipitate) as soon as they arrived in the emergency department. The results were promising in terms of the ability to correct fibrinogen levels, and so the team developed CRYOSTAT-2.
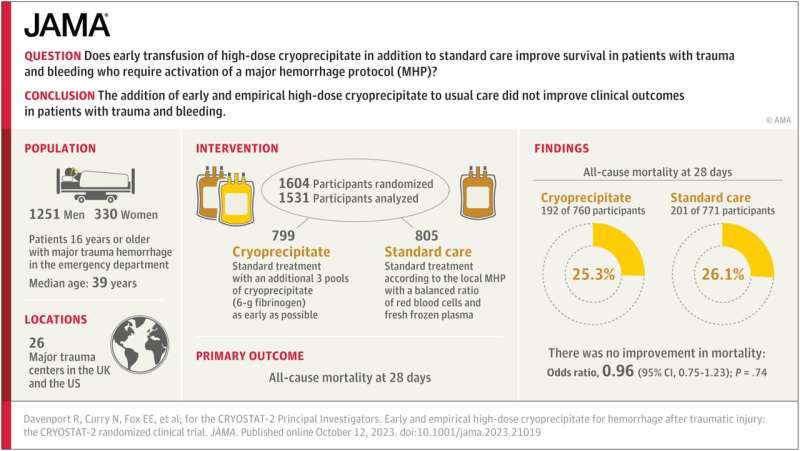
The CRYOSTAT-2 trial involved more than 1,600 patients with life-threatening injuries admitted to all 26 major trauma centers in the UK and one trauma center in the US. All participants received the standard, best practice treatments for critical bleeding, and half also received additional doses of cryoprecipitate as soon as possible after arrival.
To the researchers’ surprise, the results (published today in JAMA) showed that receiving the additional doses of the cryoprecipitate did not improve the overall survival rates of patients. Looking further, some patients appeared to do better, while some may have fared worse.
Karim Brohi, Professor of Trauma Sciences at Queen Mary, CRYOSTAT-2 Co-Chief Investigator and Consultant Surgeon at Barts NHS Trust and the Royal London, said, “Even though we were surprised by the results, they fit with our current thinking that one-size fits all does not work for trauma patients. We need to bring early diagnostic tests close to the patient in the emergency room (or even earlier at the scene of injury) to allow more precision approaches to treating severe bleeding and abnormal clotting. In other words, give fibrinogen emergently to people who need it, but not to those who don’t.”
Professor Simon Stanworth, CRYOSTAT-2 Co-Chief Investigator, Consultant Hematologist for NHS Blood and Transplant at the John Radcliffe Hospital, Oxford, said, “This large national trial answered an important question about whether there was any benefit for patients with major trauma and major bleeding when given a higher dose of blood component called cryoprecipitate as soon as possible after injury and arrival in hospital.”
“Cryoprecipitate is a source of a blood protein called fibrinogen which helps forms clots. The study was delivered across the UK as a collaboration between trauma teams, hospital blood bank laboratories and NHS Blood and Transplant Clinical Trials Unit, but unfortunately found no benefit. We need to understand the reasons for this and whether there might be some types of patients who might be helped by giving cryoprecipitate.”
More information:
Ross Davenport et al, Early and Empirical High-Dose Cryoprecipitate for Hemorrhage After Traumatic Injury, JAMA (2023). DOI: 10.1001/jama.2023.21019
Queen Mary, University of London
Citation:
Not all major trauma patients benefit from receiving additional blood-clotting factors when treating blood loss: Study (2023, October 12)
retrieved 12 October 2023
from https://medicalxpress.com/news/2023-10-major-trauma-patients-benefit-additional.html
This document is subject to copyright. Apart from any fair dealing for the purpose of private study or research, no
part may be reproduced without the written permission. The content is provided for information purposes only.